The Case of the Missing Casts
A 50 y/o woman presents with symptoms of fatigue and malaise for 1-2 weeks. Medications include ACE, HCTZ, and a multivitamin daily. She had a UTI 6 weeks ago that did not improve after a 5 day course of empiric TMP/SMX and was then given cephalexin for 10 days. Her serum creatinine was 0.7 at the time of her last doctor visit 1 year ago. Now BUN is 35 and creatinine 4.2 and UA has 1+ protein, 3+ blood, and trace leukocyte esterase with specific gravity 1.018 – CBC had no eosinophilia. ANA was 1:40 and complement C3 and C4 were normal. Exam was notable for trace LE edema and no rash.
一名50岁的女性出现1-2周的疲劳和不适症状。使用的药物包括ACE、HCTZ和每日多种维生素。她在6周前患有尿路感染(UTI),在5天的经验性TMP/SMX疗程后没有改善,然后给予头孢氨苄10天。1年前最后一次就诊时,她的血清肌酐为0.7。现在BUN为35,肌酐为4.2;尿分析为蛋白1+,血3+,微量粒细胞酯酶,比重为1.018;CBC显示无嗜酸性粒细胞增多。ANA为1:40,补体C3和C4正常。身体检查可见轻微水肿,无皮疹。
Urinary sediment showed 10-20 RBC/hpf, all of which were isomorphic. There were no acanthocytes. There were 3-5 WBC/hpf and no bacteria. Scattered tubular epithelial cells were present.
尿沉渣显示10-20个RBC/hpf,为均一性;没有棘细胞;有3-5个WBC/hpf,无细菌。存在散在的肾小管上皮细胞。
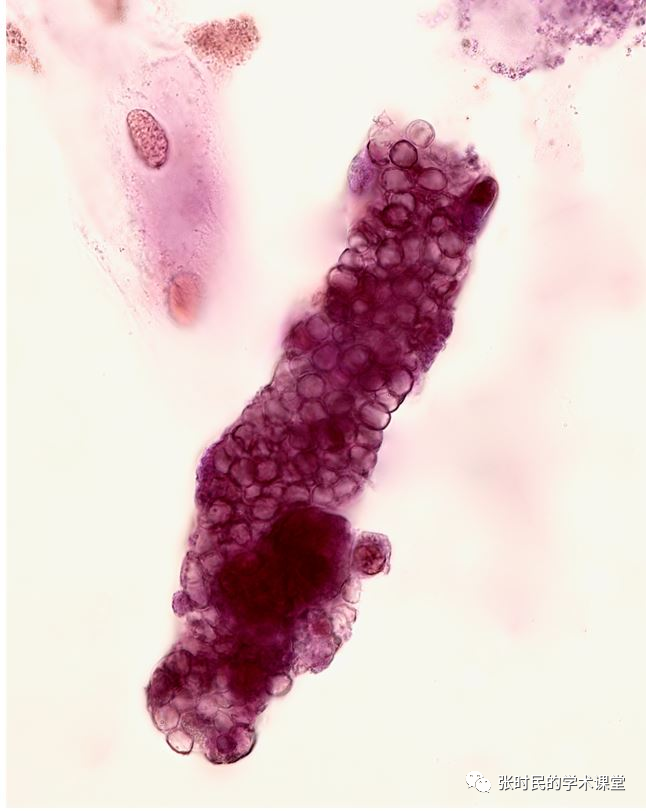
Despite the absence of acanthocytes, there were several RBC casts. There were no WBC casts.
尽管没有棘细胞,但仍有几个红细胞管型,没有白细胞管型。
图1.RBC cast with some adherent tubular epithelial cells – brightfield with Sternheimer-Malbin stain 带有一些粘附肾小管上皮细胞的红细胞管型。SM染色后的光学显微镜图2.RBC cast – brightfield with Sternheimer-Malbin stain 红细胞管型-光学显微镜加SM染色
Renal biopsy showed moderate to severe interstitial inflammatory infiltrate (monocytes and eosinophils) and acute tubular injury.肾活检显示中度至重度间质性炎性浸润(单核细胞和嗜酸性粒细胞)和急性肾小管损伤his case is a good reminder that allergic interstitial nephritis does not always present with WBC casts1. Hematuria and pyuria alone may be the most common urinary finding. Remember that red blood cells may enter the tubular lumen via damaged glomerular capillary membranes or damaged tubular basement membranes. In acute interstitial nephritis, intense inflammation may lead to disruption of interstitial vessels allowing extravasation of RBC’s into the tubular lumen via gaps in the tubular basement membrane.该病例很好地提醒我们,过敏性间质性肾炎并不总是与白细胞管型一起出现。血尿和脓尿可能是最常见的泌尿系统症状。请记住,红细胞可能通过受损的肾小球毛细血管膜或受损的管状基底膜进入管状腔。在急性间质性肾炎中,强烈的炎症可能导致间质血管破裂,使红细胞通过管状基膜的间隙外渗到管状腔中。
编者解读并注:红细胞是因炎症从破裂的肾小球毛细血管或受损的基底膜进入到肾小管内,再进入到管型内,所以红细胞没有受到挤压,没有受到损伤,是以正常形态红细胞出现在管型内。因此有这种非肾小球肾炎病人而出现红细胞管型的例外Fogazzi GB Ferrari B Garigali G Simonini P Consonni D Urinary sediment findings in acute interstitial nephritis. Am J Kidney Dis. 2012; 60: 330–332. https://doi.org/10.1053/j.ajkd.2012.05.002